Source: French to English Tester Published on: 2026-04-19
Source: The Conversation – in French– By Frédéric Blanc, Professor of geriatrics and neurologist, head of the Mobile Neuro-Psy-Research Gerontology Department and the Memory Resource and Research Center (CMRR), researcher in the IMIS team of the ICube laboratory, University of Strasbourg, University of Strasbourg
The relatives of actress Nathalie Baye announced her death on Saturday, April 18. Aged 77, she suffered from Lewy body disease. Less well known than Alzheimer’s or Parkinson’s diseases, this neurocognitive disease nonetheless affects no fewer than 250,000 people in France.
Robin Williams,Monica Vitti,Catherine Labordeor, recently,Nathalie Baye : all these personalities were taken by Lewy body disease.
This neurocognitive disease is generally only publicized when it is responsible for the death of a celebrity. However, it is common, as in France, it affects about 250,000 people, making it the second most widespread neurodegenerative disease, after Alzheimer’s disease, and placing it on the same level as Parkinson’s disease. Worldwide, it is estimated that Lewy body disease affects more than 10 million patients.
What causes it? What symptoms should raise an alert? How is it managed? Here is what you need to know.
A long-ignored disease
Lewy body disease is named after the presence, in the neurons of patients, of inclusions called “Lewy bodies,” named after the German physician Friedrich Heinrich Lewy, who first mentioned their existence in 1912.
However, it was not until 1976 that the first clinical case was formally described, while the first international clinical criteria were only defined in 1996.
At its earliest stages (thestage “prodromal” or “prodromic”, which is succeeded by the“Light” stage), Lewy body disease is characterized by the dysfunction of certain parts of the brain, such as theInsulaand theolfactory bulbs. The insula is involved in cognition, emotions, self-awareness, pain, the autonomic nervous system, taste, while the olfactory bulbs are, as their name indicates, involved in olfaction.
These dysfunctions are due to the accumulation in neurons of the abnormal form of a protein called alpha-synuclein. In its usual state, this protein adopts rather a helical conformation (also called “alpha helix”; this is the way the protein organizes itself in space). In its toxic form, its conformation changes, and the alpha-synuclein folds rather into a “pleated sheet” (a conformation called “beta sheet”).
The accumulation of these “layered” alpha-synucleins results in the creation of Lewy bodies inside neurons, throughout the course of the disease.
However, alpha-synuclein is important for the functioning of neurons. It is a key element in the regulation of synaptic vesicles (small “bubbles” filled with chemical messengers called “neurotransmitters,” which are brain hormones secreted by neurons, such as acetylcholine, noradrenaline, serotonin, or dopamine), in transmission between neurons, and in synaptic plasticity (the synapse is the contact area between two neurons).
The accumulation of the toxic form of alpha-synuclein disrupts neuronal function, as neurons are less able to secrete the synaptic vesicles that allow them to communicate with each other.
This phase (called “neurofunctional” because it affects neurotransmitters)lasts at least 15 to 20 years. Subsequently, Lewy body disease enters a more aggressive stage: not only do the patients’ neurons continue to malfunction, but moreover, some of them begin to be destroyed.
It should be noted that if Lewy bodies are also present in Parkinson’s disease, they are different from those of Lewy body disease in their appearance, their location in the brain, and theconformation of alpha-synucleinthat they contain.
What is known about the causes of Lewy body disease and its risk factors?
Some studies suggest that Lewy body disease may have environmental origins.
Chronic contact with certain toxic substances, such asphthalatesor thereair pollution (in the form of ultrafine particles), as well ascertain infections, could promote conformational changes of alpha-synuclein during aging, and trigger Lewy body disease, particularly at the level of the olfactory bulbs, which arethe only parts of the brain in contact with the outside, at the level of the nose.
Among the known risk factors for the disease areanxiety and depression. Often, it is noticed that patients suffered from depression a few years earlier; for this reason, it is believed that this pathology constitutes a mode of entry into Lewy body disease.
The other identified risk factors are arterial hypertension, diabetes, bad cholesterol, strokes, family history of Lewy body disease or Parkinson’s disease, or mutations in certain genes (notably the GBA or ApoE4 genes, which are nevertheless not the cause of the disease).
Numerous symptoms
Catherine Laborde has testified extensively about her illness: she was greatly troubled by her concentration difficulties, as well as by the cognitive and alertness fluctuations she experienced. She was also subject to great fears, without being able to explain their cause. This is a very common clinical picture of Lewy body disease.
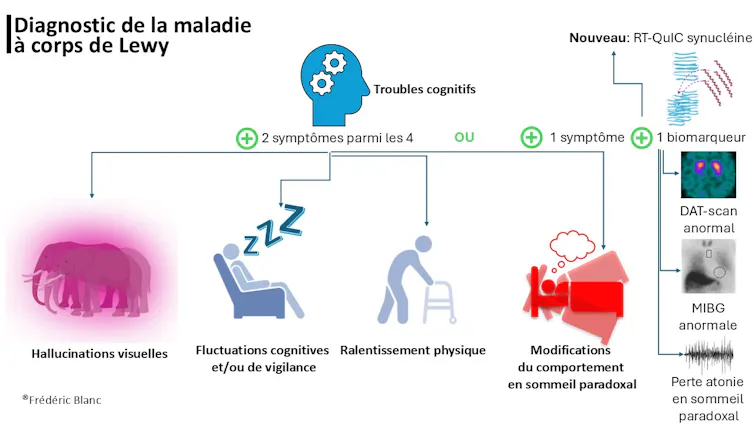
The main symptom of this condition is the presence of cognitive difficulties, which may manifest as decreased concentration, slowness, as well as difficulties in organizing oneself (referred to as “subcortical-frontal syndrome”). These cognitive difficulties are accompanied bydifferent symptoms called “cardinal” :
-
Cognitive and vigilance fluctuations that combine moments of drowsiness, long naps, fixed staring, or difficulties at certain times concentrating (the cognitive and speech difficulties experienced by Joe Biden during the televised debate with Donald Trump, which led to his withdrawal from the U.S. presidential race, should make us question cognitive fluctuations).
-
REM sleep behavioral disorders: the phase of sleep called “REM” is the phase of dreaming sleep; normally, during this phase, the body is naturally paralyzed. This is not the case for patients with Lewy body disease: some of them have restless sleep, they clearly live their dreams, start moving and shouting while they are asleep, with their eyes closed.
-
Visual hallucinations: they affect 70 to 80% of patients. In the prodromal stage (the early stage of the disease), these hallucinations consist of simple sensations of movement or presence. Then, they become true hallucinations: patients see people, animals, or scenes appearing before their eyes.
-
Parkinsonian syndrome: this most often manifests as physical slowing or stiffness of a part of the body. Unlike Parkinson’s disease, Lewy body disease is not, or very little, associated with a resting tremor of the hands.
These symptoms result from dysfunctions of neurons, and the resulting lack of neurotransmitters: the lack of acetylcholine promotes cognitive difficulties, the lack of serotonin and noradrenaline promotes depression, the lack of melatonin promotes sleep disorders, and the lack of dopamine promotes slowing down.
It should be known that it is rare for all four cardinal symptoms to be present in the same person, although it can happen: most often, patients exhibit only one or two of them.
In addition to the cardinal symptoms, many other symptoms can bother patients with Lewy body disease. Thus, it is common for patients to exhibit psychobehavioral symptoms, such as anxiety, depression, apathy (lack of motivation), or sometimes even delirium. The patient also often hasdifficulty expressing one’s emotions, or recognizing the emotions of others.
Many patients also have neurovegetative symptoms, such as a runny nose (rhinorrhea), dryness, urinary difficulties, or low blood pressure upon standing. There are also neurosensory symptoms, such as difficulties in detecting odors, or alight sensitivity.
During the most severe stages of the disease, patients lose the ability to perform daily living activities: dressing, eating, washing, using the telephone, the television remote control… Patients walk less well, lose weight, because some have difficulty swallowing.
When should one consult?
The symptoms of Lewy body disease are highly variable from one patient to another, which explains why, despite its frequency, this condition is little or not diagnosed. It is often confused with so-called “normal” aging, or with other diseases, such as Alzheimer’s disease, Parkinson’s disease, or certain psychiatric illnesses, like depression or bipolar disorder.
Patients usually consult due to cognitive disorders, such as mental slowness or difficulty concentrating. However, it is also advisable to consult when one develops depression after age 60 without an obvious reason, or if one experiences visual difficulties while the ophthalmologist’s examination is normal.
Other reasons to seek consultation: starting to sleep a lot during the day, or beginning to have severe nightmares to the point of thrashing around in bed.
Frederic Blanc,Provided by the author
In general,The diagnosis based on clinical symptoms is sufficient.. However, when necessary, additional examinations may be performed, such as a brain scintigraphy (DAT-scan, designed to highlight a decrease in dopamine activity, reflecting parkinsonian syndrome), a cardiac MIBG scintigraphy, or a sleep recording (which may show a loss of atonia during REM sleep – in other words, the loss of normal paralysis during dreams).
More recently, it has become possible to detect alpha-synuclein (a component of Lewy bodies) in the cerebrospinal fluid (which bathes the brain and spinal cord) through a sample obtained by lumbar puncture. The technique implemented, calledRT-QuIC synuclein, makes it possible to detect Lewy bodies even before the onset of disease symptoms.
We thus know, thanks to the Swedish study Biofinder, that8% of the population at 70 years old on average present Lewy bodies detected by this technique.
Research is now focused on identifying an equivalent biomarker that would work through a simple blood test.
Where are the treatments at?
There are not yet treatments to combat protein deposits known as Lewy bodies, nor to cure Lewy body disease. However, there aresymptomatic treatmentswhoimprove the presence of neurotransmitters in the brain.
Currently, it is believed that treating patients from the mild prodromal stages (the earliest stages) probably has a strong interest in preventing neuronal destruction. Indeed, combating neuronal dysfunction can undoubtedly prevent some of these neurons from dying out.
In this respect, it is probably important to treat depression and anxiety as early as possible, since they are both prodromal symptoms and risk factors for Lewy body disease.
Moreover, it is known that care provided by health professionals (speech therapist, neuropsychologist, psychologist, occupational therapist, physiotherapist, psychomotor therapist) for the purpose of cognitive or physical remediation is beneficial to patients.
The early association of these two approaches, human and medicinal, allows optimizing the quality of life of patients and thus that of their loved ones. We are fortunate to have in France a dynamic association of MCL patients and caregivers:the A2MCL. It also helps to better support patients and their relatives by providing a telephone listening service, committed psychologists, the dissemination of advice, and the sharing of experiences among caregivers.
Regarding the curative aspects, therapeutic trials are underway in France and around the world to attempt todevelop effective treatments. A promising drug is Neflamapimod, which reduces brain inflammation and promotes connections of acetylcholine neurons. Our team is also testing robot-guided transcranial magnetic stimulation, aiming to promote the reactivation of the Insula, affected from the prodromal stage. We are also evaluating the effectiveness of a neuromodulation protocol using light, with theClinatec foundation.
In conclusion, it should be emphasized that research aimed at better understanding and treating Lewy body disease is dynamic. However, while it is qualitatively excellent, quantitatively it is insufficient: in recent years, there have been 30 times fewer clinical trials on Lewy body disease than on Alzheimer’s disease. Yet, if we collectively make progress in the fight against this condition, it will greatly benefit patients, their families, and society as a whole.
To go further
- TheA2MCL association website, which supports and accompanies people affected by Lewy body disease as well as their relatives.
![]()
Frédéric Blanc is a Professor of Geriatrics at the University of Strasbourg, and a Hospital Practitioner, Geriatrician and Neurologist at the Strasbourg University Hospitals. He is the chairman of the scientific committee of A2MCL, which is the reference association for Lewy Body Disease (LBD). He is a member of the operational committee of the Alzheimer Foundation and he is a member of the operational committee of E-DLB (which brings together all research teams on LBD).
His team and he himself have received funding from the inter-regional PHRC, the national PHRC, Vaincre Alzheimer, the Alzheimer Research Foundation, France Alzheimer, and the A2MCL.
He was the coordinator for France of the Delphia trial by Eisai for MCL. He is the coordinator for France of the Neflamapimod trial by EIP Pharma.
–ref. Lewy body disease: what is this common but little-known neurocognitive illness that took Nathalie Baye?https://theconversation.com/lewy-body-disease-what-is-this-common-yet-little-known-neurocognitive-disorder-that-took-nathalie-baye-248597